


- Weight: 100 kg
- Height: 185 cm
- BMI: 29
- hyperomocysteinemia
- reduced glucose tolerance
- history of Hodgkin Lymphoma treated with chemotherapy and radiotherapy
- thoracic outlet syndrome
- pectus excavatum
- ulcerative colitis
- allergic asthma
- Hb: 14.6 g/dl
- Creatinine: 1.08 mg/dl
- eGFR: 118 ml/min
- LDL 145 mg/dl
- Lp(a) 8 mg/dl
- PLT 386. 000/ul
- hsTnI 863,6 pg/ml
- Mesalazine 1200 mg twice daily
- STEMI - Inferior
- Improvement of symptoms after optimized medical therapy (IV nitrates and beta-blockers).
- Development of fever; blood cultures positive for Staphylococcus epidermidis, targeted IV antibiotic therapy initiated.
35 years old, male
Cardiovascular Risk Factors:
Medical History:
Lab Test
Admission Medical Therapy
ECG
Transthoracic Echocardiogram
Moderately dilated left ventricle with infero-posterior and basal infero-septal akinesia.
LVEF estimated at 35-40%
Moderate to severe functional mitral regurgitation.
Coronary Angiography
Acute thrombotic total occlusion of the mid right coronary artery.
Chronic total occlusion of mid left anterior descending and proximal left circumflex.
Primary PCI of Right Coronary Artery
Primary PCI and direct implantation of two overlapping DES (Onyx Frontier 2.5 x 30 mm and Onyx Frontier 3.0 x 12 mm).
Baseline
Post-stenting
Clinical Course and Heart Team Discussion
Coronary Care Unit stay
- Staged percutaneous revascularization of both CTOs was favoured after multidisciplinary evaluation.
- The decision was driven by prior mediastinal irradiation and associated surgical risk due to mediastinal fibrosis, impaired wound healing, hostile chest anatomy, increased perioperative morbidity.
- Conventional risk scores likely underestimate operative risk in radiation-exposed patients (STS morbidity and mortality risk score 7.64%, Euroscore II 1.31%).
- From a long term perspective in this 35-year-old patient, concerns regarding venous graft durability and the cumulative lifetime risk of repeat sternotomy further supported an upfront percutaneous strategy, thereby preserving CABG as a future option,
- Cardiac MRI deemed essential to characterize myocardial viability, presence and distribution of ischemic scar before any revascularization.
- Metoprolol 100 mg ½ BID
- Mesalazine 1200 mg BID
- Isosorbide Mononitrate 50 mg OD
- Acetylsalicilic Acid 100 mg OD
- Ivabradine 5 mg OD
- Atorvastatin 80 mg OD
- Pantoprazole 40 mg OD
- Sacubitril/Valsartan 49/51mg BID
- Empagliflozin 10 mg OD
- Furosemide 25 mg OD
- Spironolactone 25 mg OD
- Ticagrelor 90 mg BID
Non-Invasive Imaging
Cardiac MRI showed ischemic injury pattern with myocardial edema in the mid-basal infero-septal wall (T2 hyperintensity).
Subendocardial LGE involving infero-septal and anteroseptal segments (basal to apical).
Evidence of no-reflow in the mid-basal septum.
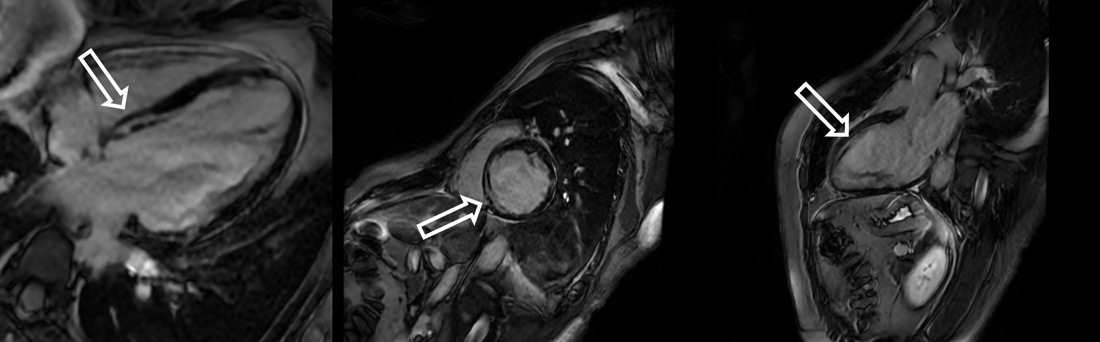
Cardiac MRI
TOE showed post-infarction cardiomyopathy with mildly reduced left ventricular ejection fraction (LVEF 40-43%).
Persistent moderate-to-severe functional mitral regurgitation due to posterior leaflet tethering and anterior leaflet sliding.
No vegetations or structural findings suggestive of infective endocarditis.
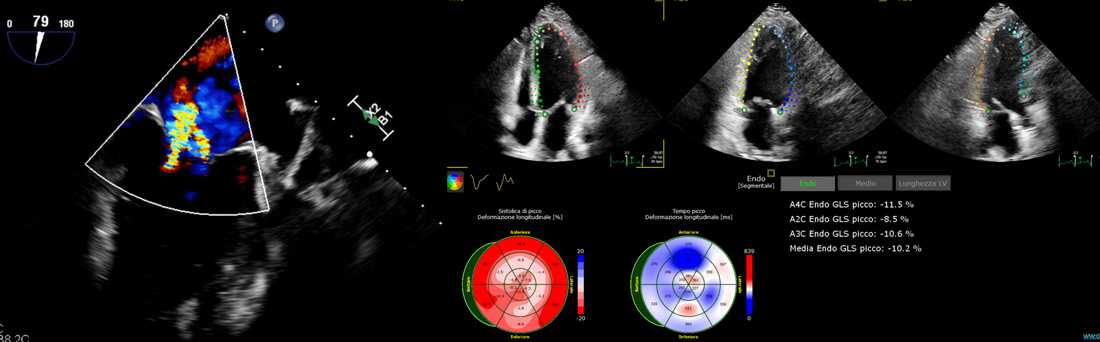
TOE
Left Anterior Descending CTO PCI
Dual injection (right radial and right femoral). EBU 3.75 6 Fr. Finecross Microcatether. Unsuccessful crossing attempts with Sion Blue and Whisper wires and final successful crossing with Gaia III, then exchanged for a BMW wire. Predilation with 1.5 x 15 mm and 2.5 x 15 mm semi-compliant balloons. PCI of left anterior descending-first diagonal bifurcation with stepwise provisional approach. Implantation of two Xience DES (2.75x23 mm and 3x28 mm, distal to proximal, respectively, overlapping), followed by POT-Kiss-POT. Optimal TIMI flow at completion.


Follow up
Medical therapy
Left ventricle of normal dimensions and wall thickness (LVEDD 53 mm, IVSd 10 mm, PWd 10 mm). Moderately reduced systolic function (LVEF 45%) with inferoposterior akinesia and hypokinesia of the mid-distal interventricular septum. Grade II diastolic dysfunction (E/e′ 9). Mild-to-moderate mitral regurgitation. Right heart chambers within normal limits (TAPSE 20 mm). Mild tricuspid regurgitation; estimated PAPs 25 mmHg.
- Prior mediastinal irradiation promotes premature, multivessel coronary artery disease and valve dysfunction, and creates a hostile surgical substrate, making standard risk stratification potentially misleading in young cancer survivors.
- In STEMI with multivessel disease, culprit-only PCI followed by staged complete revascularization aligns with contemporary guideline recommendations.
- Multidisciplinary Heart Team evaluation is critical to tailor the revascularization strategy beyond conventional risk scores, integrating prior radiation exposure, anatomical complexities and lifetime management.
- Cardiac MRI-based viability assessment remains pivotal to ensure appropriate selection of patients undergoing complex CTO intervention.
- Functional mitral regurgitation and post-infarction left ventricular dysfunction require careful longitudinal follow-up to reassess recovery after revascularization and GDMT optimization.
- Persistent left ventricular impairment or moderate–severe mitral regurgitation should prompt early referral to advanced heart failure care—particularly important in patients with prior thoracic irradiation who carry additional procedural and prognostic challenges.
None
Disclaimer
This case report and/or content does not reflect the opinion of iHF or iheartfunction.com, nor does it engage their responsibility.
