Why this study – the rationale/objective?
Heart failure with preserved ejection fraction (HFpEF) remains associated with a substantial residual risk of adverse outcomes, while effective disease-modifying therapies remain limited. One major challenge remains the marked biological and clinical heterogeneity of the syndrome, which likely contributes to the neutral or modest effects observed across several pharmacological trials. Increasingly, HFpEF is being recognized as a constellation of distinct phenotypes characterized by different pathophysiological mechanisms and potential therapeutic target, emphasizing the need for more individualized treatment strategies.
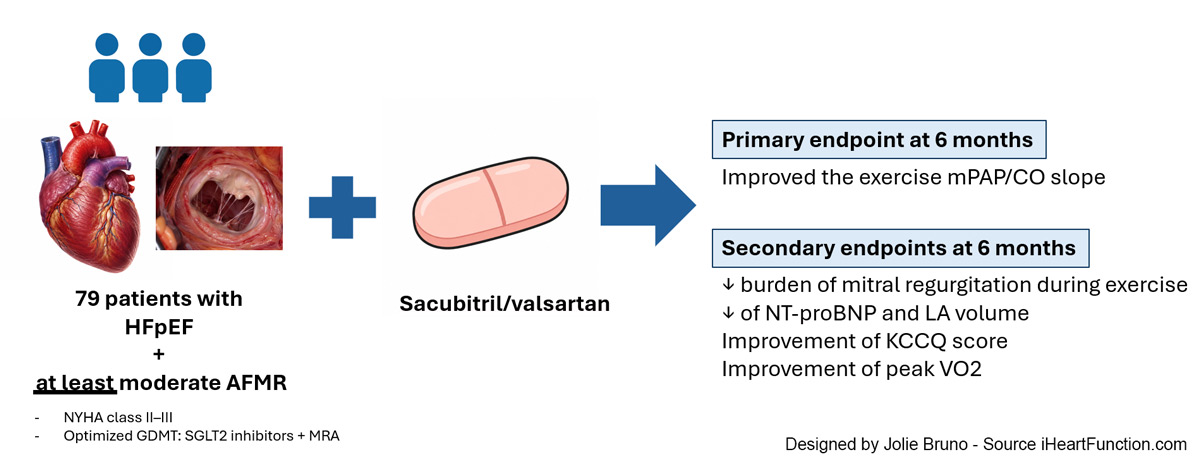
In this context, Dhont et al in the PRAISE-MR trial recently presented at the 2026 ESC Heart Failure Congress and simultaneously published in Circulation, investigated a particularly relevant HFpEF phenotype: patients with atrial functional mitral regurgitation (AFMR). The study evaluated whether angiotensin receptor–neprilysin inhibition (ARNI), i.e. sacubitril/valsartan, could improve haemodynamic and functional status
How was it executed – the methodology?
PRAISE-MR was an investigator-initiated, prospective, multicentre, randomized, open-label trial with blinded assessment of the primary endpoint. Symptomatic patients with NYHA class II–III HFpEF, defined by a left ventricular ejection fraction ≥50%, and at least moderate AFMR, documented within 1 year, were enrolled. Importantly, all participants were already receiving optimized background therapy, including SGLT2 inhibitors and mineralocorticoid receptor antagonists.
Patients were randomized in a 1:1 fashion to receive sacubitril/valsartan in addition to standard of care or standard therapy alone. ARNI therapy was initiated at 24/26 mg twice daily and uptitrated every two weeks to the maximally tolerated dose. Rhythm-control strategies for atrial fibrillation, when indicated, were established prior to enrolment. Comprehensive assessment was performed at baseline and after 6 months, including combined cardiopulmonary exercise testing (CPET) and echocardiography, alongside ambulatory blood pressure monitoring.
The primary endpoint was the change in exercise mPAP/CO slope, a flow-adjusted marker of pulmonary vascular, from baseline to 6 months. Secondary endpoints included resting and exercise-related AFMR severity, left atrial volume and function, NT-proBNP levels, Kansas City Cardiomyopathy Questionnaire (KCCQ) score, peak VO2, and VE/VCO2 slope.
What are the main findings?
A total of 79 patients completed the study, with a slower-than-anticipated enrolment. Notably, the trial was characterized by a 6% dropout rate. Baseline clinical, echocardiographic, and exercise-related characteristics were well balanced between treatment groups. Compared with standard therapy alone, sacubitril/valsartan significantly improved the exercise mPAP/CO slope, with findings remaining robust across multiple multivariable sensitivity analyses. Although overall changes in AFMR severity did not significantly differ between groups, patients receiving ARNI therapy exhibited a lower burden of mitral regurgitation during mid-exercise. In parallel, sacubitril/valsartan was associated with significant significant reduction in NT-proBNP and LA volume, as also improvements in health status, as reflected by KCCQ score, and exercise capacity, assessed by peak VO2. By contrast, no significant effect was observed on the VE/VCO2 slope.
Critical reading and clinical implications
The pathophysiological rationale supporting ARNI therapy in HFpEF appears biologically compelling. Through simultaneous neprilysin inhibition and blockade of the renin–angiotensin–aldosterone system, sacubitril/valsartan enhances natriuretic peptide activity while attenuating vasoconstriction, myocardial fibrosis, hypertrophy, and sodium retention. Collectively, these mechanisms may improve ventricular compliance, reduce filling pressures, and optimize ventricular–arterial coupling, potentially through effects extending beyond blood pressure reduction alone.
Such mechanisms provide a plausible biological framework for the observed findings. Nevertheless, several uncertainties remain. Previous studies evaluating the impact of ARNI therapy on atrial remodelling have yielded inconsistent results. In the PARABLE trial, sacubitril/valsartan was associated with increased left atrial volumes in pre-HFpEF patients, although the clinical relevance of this finding remained uncertain. Conversely, subsequent meta-analytic evidence suggested reductions in left atrial volume as also in left ventricular mass index, potentially indicating favourable reverse remodelling. Importantly, concomitant rhythm-control strategies and background guideline-directed medical therapy (GDMT) may have contributed to the observed effects through synergistic and additive interactions, particularly in terms of decongestion in this case. However, the specific atrial fibrillation treatments received by patients were not detailed, nor was it clearly reported whether GDMT remained unchanged throughout the 6-month follow-up.
Overall, PRAISE-MR provides important mechanistic and functional insights into a highly selected HFpEF phenotype. However, whether these favourable physiological effects ultimately translate into meaningful improvements in hard clinical outcomes remains uncertain. Larger and longer-term studies are therefore warranted to better define the prognostic role of ARNI therapy in patients with AFMR-associated HFpEF and, more broadly, to advance a phenotype-oriented therapeutic approach in HFpEF.

