

- Left ventricular hypertrophy
- Hypokinesia of the basal inferior, posterior, and septal segments; hypokinesia of the mid-lateral and mid-posterior segments
- Eccentric mitral valve insufficiency of grade I–II
A 60-year-old male patient (170cm, 84kg, BMI 29kg/m²) with a history of type 2 diabetes mellitus presented for follow-up of known myocardial dysfunction. He reported mild symptoms, including reduced exercise tolerance. Given his risk profile – including dyslipidemia, family history of coronary artery disease, and diabetes - a coronary angiogram was recommended.
His past medical history included:
Type 2 Diabetes Mellitus, onset in 2021
HbA1c 7% under medication with Metformin and Abasaglar
Suspected diabetic polyneuropathy
Bilateral mediasclerosis
Current echocardiographic findings:
Aortic sclerosis with a small plaque
Cardiovascular risk factors (CVRF): Dyslipoproteinemia, family history of coronary artery disease (CAD)
Small axial hiatal hernia
Medications:
Meformin: 500 mg 1-0-1
Abasaglar: 0-0-0-14IE
Semaglutid (was added currently): 0,25mg s.c.1x per week
Atorvastatin 20mg: 0-0-1
Ranexa 375mg: 1-0-1
Vit. D 2000IE: 1-0-0
Angio and echo
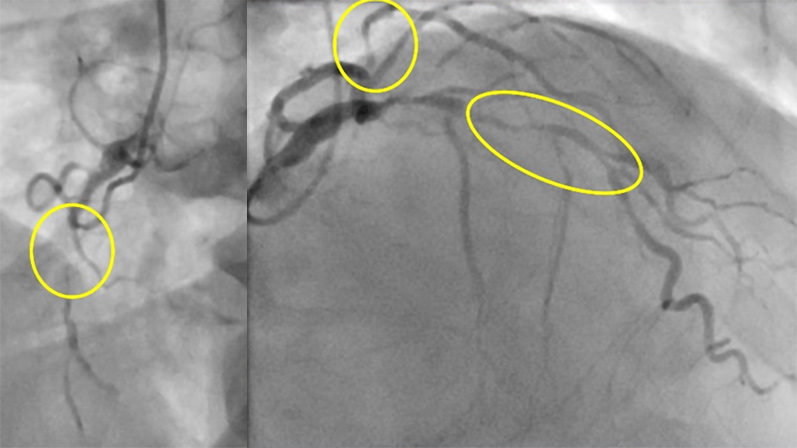
Coronary angiography revealed a severe three-vessel disease with severe proximal LAD stenosis, severe proximal circumflex artery stenosis, and RCA occlusion with retrograde perfusion (10th June 2025). Echocardiography showed a mild left ventricular hypertrophy, ejection fraction 43%, very eccentric mitral regurgitation (uncertain grading).
- Proximal LAD stenosis (Class IA recommendation for revascularization)
- Three vessel disease with diabetes mellitus (Class IA recommendation for CABG vs PCI)
- Low surgical risk (EuroScore II 1.18%)
Our patient met the criteria for surgical coronary revascularization:
He was scheduled for CABG and received an intraprocedural TEE, that revealed severe mitral regurgitation due to some restriction but also a deep indentation between P1 and P2:
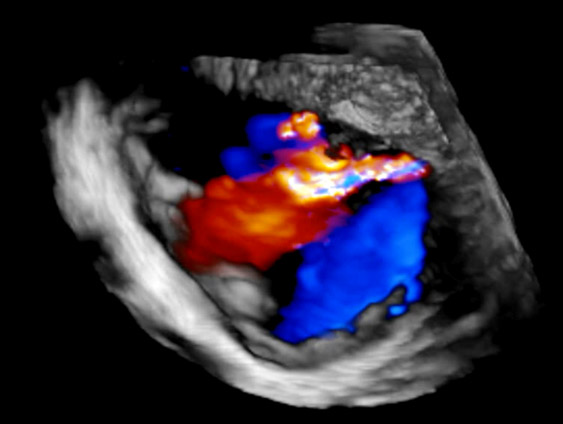
He received total arterial grafting with LIMA to LAD and RIMA as a t-Graft to the marginal branch and to RIVP. In addition, a mitral repair was performed with reduction annuloplasty with a Physio II 30mm ring and suture for closure oft he indentation between P1 and P2 and a commissural suture to approximate P1 and A1.
His postoperative course was uneventful. Discharge echo revealed a left ventricular ejection fraction of 50% and no residual mitral regurgitation, mitral gradient 2mmHg.
- Intraprocedural TEE can uncover the true severity of valve lesions not apparent in preoperative transthoracic imaging.
- Mitral valve repair for functional regurgitation can result in excellent outcomes, but:
- Predictors of recurrence are not well established.
- In elderly patients or those with complex mitral anatomy (e.g., short/restrictive posterior leaflet), valve replacement may be preferred.
- Concomitant mitral surgery during CABG is Class IB recommended in patients with moderate-to-severe functional MR to improve outcomes.
- Diabetes with three-vessel disease favours CABG over PCI due to long-term survival and event reduction benefits.
- Total arterial revascularization, when feasible, provides better long-term patency and outcomes compared to vein grafting.
Semaglutide initiation aligns with current guidelines recommending GLP-1 receptor agonists in diabetic patients with high CV risk.
Disclaimer
This case report and/or content does not reflect the opinion of iHF or iheartfunction.com, nor does it engage their responsibility.
